Most healthcare organizations don't have an automation problem. They have a process problem. The scheduling workflow that generates complaints every Monday isn't broken because the software is wrong. It's broken because nobody documented how it actually runs - only how it's supposed to run. And those two things stopped matching somewhere around 2019.

Business process management in healthcare is how you close that gap. Not by buying a platform. By treating processes as something worth understanding, measuring, and deliberately improving before you automate anything.
The part teams learn late
- BPM is a management discipline first - software is one tool that supports it, not a synonym for it.
- The four-phase cycle (identify, document, analyze, improve) breaks when teams skip directly to redesign.
- BPM applies to clinical workflows, not just billing and scheduling.
- Staff involvement in documentation isn't a change management nicety - it's the variable most implementations underestimate.
What Business Process Management in Healthcare Actually Means
Business process management is a structured method for understanding, documenting, modeling, analyzing, simulating, executing, and continuously improving end-to-end processes inside a healthcare organization. That definition comes from peer-reviewed literature, not a vendor website, and the sequence in it matters. Understanding and documenting come before executing. Analysis comes before improvement.
The common misread is that BPM means workflow software. It doesn't. Software can support BPM, but a healthcare organization that buys a BPM platform without first working through its process modeling hasn't implemented BPM. It's installed a tool on top of an undocumented process and called it managed.
What BPM actually does is shift the organization's attention to business processes as objects worth managing at a higher level than individual tasks. That means consistent documentation, defined indicators, performance measurement, and a continuous improvement loop. In a hospital setting, those business processes span everything from patient admission to medication recording to billing reconciliation. The discipline applies equally across all of them.
Why BPM Gets Misread as Just Another Automation Tool
The confusion is understandable. Vendors selling BPM software market it as the thing that fixes inefficient workflows. So teams buy bpm software, plug it into their systems, and discover three months later that the workflow is still inconsistent - it's just inconsistent faster now.
What BPM methodology actually addresses is the reason workflows became inconsistent in the first place: siloed systems, undocumented handoffs, and no shared definition of what "done" looks like at each process step. A 2025 PMC review on applying robotic process automation to monitor business processes in healthcare identified exactly this gap - BPM has established process-integration patterns in healthcare, but has not been effective at guiding process redesign. That's not a software limitation. It's what happens when organizations skip the analysis phase and jump to execution.
Effective business process management treats workflow as a management discipline, not a procurement category. It supports standardization across care settings, defines indicators for measuring process performance, enables benchmarking against those indicators, and creates the foundation for operational excellence. Automation software, when it appears at all, is one mechanism for executing a well-designed process. It can't substitute for the design work itself.
That is where the ticket usually starts.
🤔 Wait.
Most teams purchase a BPM system before they've documented what their current processes actually do. But BPM methodology says documentation is the second step, immediately after identification. Buying the tool first inverts the sequence and nearly guarantees that the BPM lifecycle starts broken. The software can't map a process the organization hasn't yet described.
The Four Phases of BPM Implementation in a Hospital Setting
The four-phase sequence that appears in rigorous hospital case studies isn't a vendor roadmap. It's the practical mechanism behind BPM: identify processes, document them, analyze and measure them, then improve them. The sequence is not interchangeable.
Teams that skip documentation and move directly to improvement are redesigning a process they don't yet understand. Teams that skip analysis and move directly to improvement are optimizing against assumptions rather than data. Both patterns produce the same outcome: a BPM effort that stalls at the first obstacle because nobody can agree on what the process is supposed to do, let alone whether it's doing it.
Identifying and Documenting the Processes That Actually Run the Hospital
Identification means naming the processes that genuinely affect operations and patient outcomes: admission, discharge, medication discounting, drug recording, patient scheduling, billing review. These are the processes that appear in hospital case studies precisely because they are the ones where variation creates the most visible downstream damage.
Documentation is where the work gets uncomfortable. The business process model that gets committed to paper is almost always the idealized version - how the process should run when everything goes right. The process that actually runs is something messier, with workarounds, undocumented exceptions, and steps that belong to whoever happened to be on shift that day. When the documentation captures the ideal and ignores the actual, everything built on top of it inherits that gap. Business process model and notation (BPMN) tools help make this concrete, but the underlying discipline is observation and honesty about what's real, not just what's intended.
A good test: ask two people from different shifts to walk through the same healthcare process. If the descriptions diverge significantly, the documentation phase has work left to do.
Analyzing, Measuring, and Then Improving - Not the Other Way Around
Analysis means establishing baseline indicators before any redesign decisions are made. How long does patient discharge take on average? Where do delays cluster? Which handoff points generate the most errors? A 2022 review published on PMC found that process-based management in hospital settings can improve efficiency, reduce waste, add value, and contribute to better financial results - but only when measurement precedes improvement decisions. That conditional is doing real work in that sentence.
The most common mistake in this phase is jumping to redesign after identification, treating documentation as complete when it's just descriptive. Optimize business processes means something specific: change a defined, measured process to make it perform better against a stated indicator. Without a baseline, there's no "better." There's just different, and different without measurement is indistinguishable from worse.
Process performance data collected here also serves a second function: it makes the improvement case to the clinical and administrative staff who will need to adopt whatever changes come next. Numbers about the current state are more persuasive than opinions about it.

BPM Use Cases in Healthcare: Where It Actually Changes Outcomes
The practical case for BPM in healthcare doesn't live in a theory document. It lives in the specific places where inconsistent or poorly-designed processes cause patients to wait longer, staff to redo work, and organizations to absorb costs they don't measure. Here's where BPM has documented applications across both clinical and administrative domains.
Hospital Operations: Admissions, Discharge, Scheduling, and Billing Workflows
Hospital admissions and discharge are the two processes where BPM returns appear fastest, because the variation in those workflows is visible almost immediately. When there's no standardized admission process, bed assignment delays ripple into ED throughput, surgical scheduling, and staff allocation simultaneously. The same PMC hospital case study that documented medication discounting and drug recording workflows found that formalizing these processes with consistent handoff documentation reduced the variation that causes exceptions to become the rule.
Patient scheduling is a specific pain point in healthcare operations. The problem isn't usually the scheduling software - it's that the scheduling process hasn't been documented at the level that would let automation do anything useful. I keep seeing this in healthcare teams: the scheduling workflow runs differently for different departments, across different healthcare facilities, with different staff, and nobody has reconciled those variants into one process that could be measured. A 2025 NIH review on AI in healthcare noted that automation can reduce wait times in scheduling, billing, and triage - but the efficiency claim depends on whether the scheduling process itself is defined well enough to automate. Healthcare workflows that run in parallel variants don't benefit from automation; they just produce inconsistency at higher speed.
Billing is where undocumented process variation shows up as direct financial exposure. When the billing workflow depends on individual discretion rather than defined steps, exceptions slip through, not because staff are careless, but because there's no agreed definition of what "complete" looks like at each step.
Clinical Workflow Standardization and Reducing Handoff Errors
The misconception that BPM applies only to administrative back-office work is worth addressing directly. The same rigorous methodology used on billing and scheduling also applies to clinical and administrative processes: care delivery, care coordination, medication management, clinical triage, and handoff documentation between clinical teams.
Handoff errors are where the clinical application of BPM is most concrete. When care passes from one team to another - shift change, transfer between units, discharge to home or another facility - the information that needs to travel with the patient depends on a process. If that process isn't documented or measured, the handoff depends on the habits of whoever is present, which means patient care quality varies with staffing. BPM doesn't replace clinical judgment in that moment. It designs the process around the judgment call so the clinician has what they need to make it.
Electronic health record systems generate enormous amounts of data about clinical processes, but accessing that data as process performance information requires the process to be defined first. BPM provides the structure that makes EHR data interpretable as evidence of how care was delivered, not just as a record that something happened.
A PMC review on RPA and business process monitoring in healthcare confirmed that BPM is feasible and useful for optimizing clinical processes specifically, not just administrative ones. That finding matters because it reframes where hospitals should be looking when clinical workflow delays generate complaints.
Compliance, Quality Indicators, and Process Auditability
Healthcare regulations don't just specify outcomes. They specify documentation requirements for the processes used to reach those outcomes. BPM creates exactly the kind of process record that compliance teams need: documented steps, defined responsibilities, measurable indicators, and an audit trail that shows how the process ran on a given date.
Quality of care measurement depends on having processes consistent enough to compare. A quality indicator that measures time-to-treatment means something only when the treatment process runs the same way across people and shifts. BPM creates that consistency, which makes quality indicators meaningful rather than anecdotal. The PMC research linking BPM to standardization and benchmarking in hospital management points to this mechanism: standardization precedes measurement, and measurement precedes genuine improvement in healthcare services.
For compliance teams specifically, BPM also reduces the cost of audit preparation. When processes are documented and measured continuously, the evidence base for compliance review exists as a byproduct of normal operations.
On the automation side: when a team has completed the documentation and analysis phases and identified a stable, well-defined clinical or administrative workflow, that's where a tool like Latenode fits naturally. For something like intake routing or exception flagging, Latenode can watch process events across multiple connected systems, use built-in AI models to classify exception text or triage notes, and surface anomalies to the right queue without manual status chasing. The built-in RAG is useful when routing decisions depend on internal SOPs or policy PDFs - you upload the document directly rather than managing a separate vector database. The point is that the automation step is downstream of the BPM work, not a replacement for it.
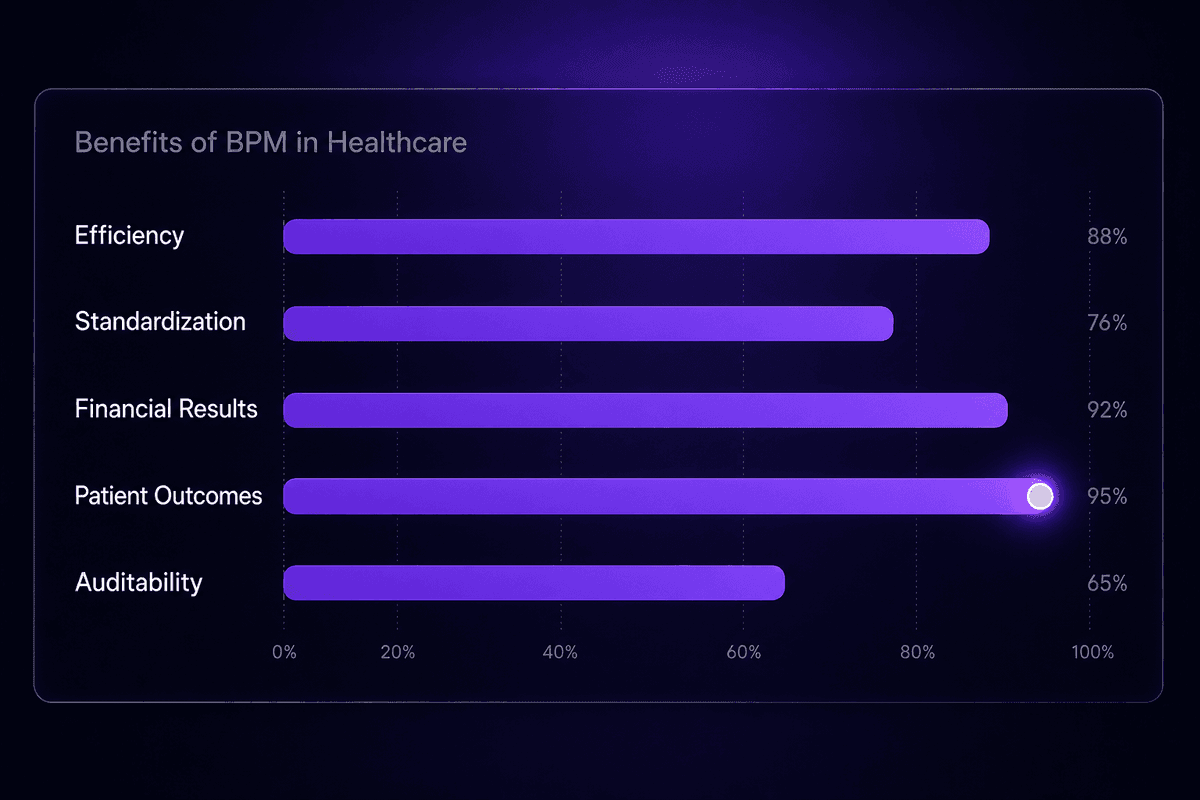
Benefits of BPM in Healthcare Beyond Generic Efficiency Claims
The research-backed case for improving healthcare through BPM is more specific than "things run better." Each benefit has a mechanism. Here's what the evidence actually says, with the "why" attached.
- Efficiency improvement through waste reduction: When processes are documented and measured, unnecessary steps become visible. In hospital settings, this typically surfaces in admission and discharge delays where redundant checks or undocumented handoffs consumed time without adding clinical value. Elimination is only possible after identification.
- Reduced process variation and its downstream costs: Inconsistent processes produce inconsistent outcomes, which generates rework, complaints, and compliance exposure simultaneously. Standardization through BPM doesn't reduce staff autonomy - it reduces the variation that creates unpredictable patient outcomes across shifts.
- Better financial results through process-level management: The PMC research on BPM in hospital management found links between process-based management and financial performance. The mechanism is specific: when processes are measured, the cost of inefficiency becomes visible and addressable, rather than absorbed invisibly as overtime or rework.
- Improved patient outcomes from better care coordination: BPM applied to clinical and administrative processes reduces handoff errors, shortens delay intervals in care delivery, and creates the documentation infrastructure that lets clinical teams see what happened in the previous step before they take the next one. Better information at handoff points improves patient care quality directly.
- A foundation for meaningful benchmarking: One of the benefits of BPM that doesn't appear in vendor brochures is the ability to benchmark against your own process history. Before BPM, there's nothing stable enough to compare. After BPM, you can measure whether last quarter's discharge process ran better or worse than this quarter's, and why.
- Support for the future of healthcare operations: A 2025 PMC article on digital readiness in palliative home care framed BPM as the bridge between operational policy and usable digital workflows. That framing matters because the healthcare system is adding digital tools faster than it's adding the process foundations those tools require to work.
What Makes BPM in Healthcare Hard to Get Right
The evidence base for BPM in healthcare is positive. The evidence for BPM implementation going smoothly is more mixed. Those two things can both be true at once, and conflating them is how organizations end up disappointed by a discipline that works - when applied correctly.
Why Staff Involvement Is the Variable Most Teams Underestimate
The PubMed systematic review on BPM feasibility in healthcare is careful about one finding: feasibility depends on staff involvement during process documentation and design. That's not a general change management observation. It's a specific mechanism.
When frontline healthcare teams aren't involved in documenting the processes they run, the documentation captures the process as management understands it, not as it runs. The gap between those two versions is exactly where BPM implementations stall. The redesigned process doesn't match the actual environment. The software built around the redesign requires workarounds from day one. Staff stop using the documented process because the documented process doesn't reflect their reality. And then the organization concludes that BPM doesn't work in healthcare.
I've seen this pattern enough that it stops being surprising. The organizations that get BPM right treat the documentation phase as an investigation, not a transcription. Healthcare teams who actually run the process are interviewed. Exceptions are surfaced, not smoothed over. The uncomfortable variants make it into the model. The business processes that result are harder to document and easier to improve, which is the right trade.
Where BPM Software and BPM Methodology Part Ways
A bpm system, a bpm platform, a bpm solution - these are tools. BPM is a management practice. The distinction matters because purchasing a bpm software product and deploying a bpm platform does not automatically change how an organization manages its processes. The methodology has to precede the tooling, not arrive with it.
What a business process management system genuinely provides is support for the execution and monitoring phases of a well-defined process. When a process has been identified, documented, and analyzed - when someone knows what it's supposed to do and has measured what it actually does - a BPM platform can enforce consistency, capture execution data, and surface deviations for review. That's valuable. But the same platform pointed at an undocumented process captures noise, not signal. The research put it plainly: BPM helps healthcare organizations focus on processes at a higher management level. Software doesn't do that focusing. People do. The bpm solution supports the work; it doesn't do the work.
📊 In practice:
A PubMed study on robotic process automation and business process monitoring in healthcare confirmed that BPM and RPA are feasible for automating tasks and optimizing clinical processes - but the finding came with a condition: outcomes depend on adequate technological support and meaningful staff involvement. Both dependencies. Neither optional. Feasibility without those conditions is just potential.
BPM Tools and Process Automation in Healthcare: What to Evaluate
Selecting a bpm tool for the healthcare industry isn't primarily a features conversation. It's a sequencing conversation. The most important question when evaluating any bpm or business process automation product isn't what it can do - it's whether your team has done the process work that would make those capabilities useful.
With that context, here's what actually matters when evaluating a healthcare business process management solution:
Process fit before feature breadth. A BPM platform should support the specific workflows your documentation phase has identified: patient scheduling, intake routing, medication management, billing reconciliation. Business process management software that's broad but doesn't map to your documented process models creates adoption friction from day one.
Interoperability with healthcare data standards. Healthcare workflows depend on HL7 and Fast Healthcare Interoperability Resources (FHIR) compatibility. Any business process automation tool that handles patient data needs to work within those standards, not around them. A scheduling process automation that can't consume or produce HL7-compliant messages creates integration debt immediately. This is not a theoretical concern - Stack Overflow has years of threads where teams discovered mid-build that their chosen platform's scheduling integration didn't include financial fields in HL7v2 scheduling messages, which is a fundamental gap for billing-linked workflows.
Staff adoption readiness over technical sophistication. Healthcare providers include clinicians, administrators, billing teams, and operations staff with widely varying technical backgrounds. A bpm solution that requires engineering resources to maintain will create ownership gaps as soon as the person who built it stops being available. Evaluate for maintainability by the team that will run it, not the team that will build it.
Process modeling and monitoring visibility. The tool should support process modeling natively - ideally with BPMN notation - and provide execution monitoring that surfaces failures, delays, and exceptions where the team that owns the process can see them. Not just in an engineering dashboard. In a format healthcare operations staff can act on.
Demonstrated support for clinical and administrative workflows, not just back-office automation. Some process automation tools are optimized for CRM or marketing workflows and adapted for healthcare. The evaluation question is whether the tool has specific support for healthcare operations, encounter orchestration, and clinical workflow routing - or whether you'll be building significant custom logic to handle healthcare-specific edge cases. The complexity of encounter creation in systems like Epic is a useful test: a workflow that requires assembling patient, account, coverage, consent, and encounter records across multiple APIs is not a simple automation. A platform that treats it as one will break in visible ways.

